आयुर्वेदिक डॉक्टर से प्रश्न पूछें और निःशुल्क या भुगतान मोड में अपनी चिंता की समस्या पर ऑनलाइन परामर्श प्राप्त करें। 2,000 से अधिक अनुभवी डॉक्टर हमारी साइट पर काम करते हैं और आपके प्रश्नों का इंतजार करते हैं और उपयोगकर्ताओं को उनकी स्वास्थ्य समस्याओं को हल करने में प्रतिदिन मदद करते हैं।
मुफ्त! आयुर्वेदिक डॉक्टरों से पूछें 24/7
Body DetoxEar, Nose, and Throat DisordersGeriatrics & RejuvenationImmunodeficiencyInfertility TreatmentNutritionOrthopedic DisordersPediatricsRespiratory DisordersSexually Transmitted Diseases (STDs)Surgery RecoveryUrological DisordersVascular DisordersDental DisordersEndocrinological DisordersGastrointestinal DisordersYoga TherapyGeneral MedicineAllergic DisordersCardio DisordersGynecology and ObstetricsCosmetologySkin and Hair DisordersEye DisordersInfectious DiseasesMental DisordersNeurological DisordersOncologyPanchakarmaSexual Health & DisordersSports Medicine
पर प्रकाशित 10/14/24
(को अपडेट 06/20/26)
2,922
Liver & Gall
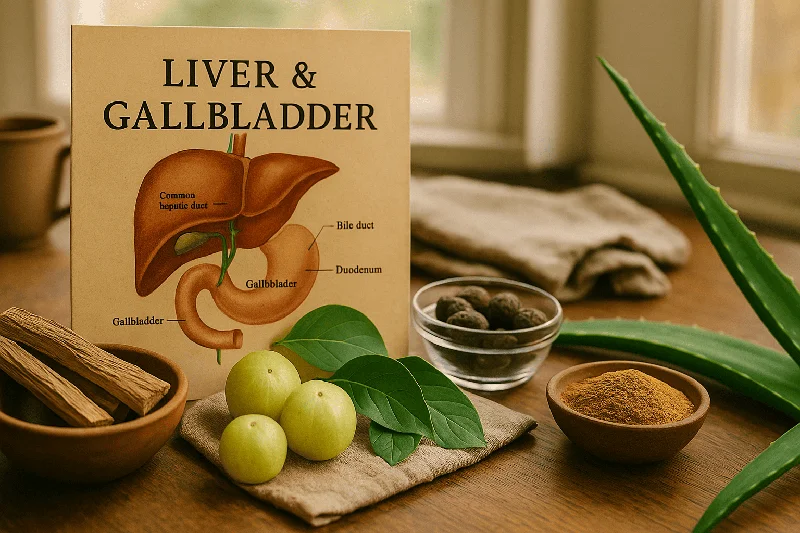
The liver and gallbladder are two deeply interconnected organs that form the core of your biliary system — yet most people don't realize just how tightly their fates are linked. The liver, your body's largest internal organ, produces bile, detoxifies blood, synthesizes proteins, and stores essential vitamins. The gallbladder, a small pear-shaped sac tucked beneath the liver, stores and concentrates that bile until your body needs it for fat digestion. When one organ struggles, the other almost always suffers. This article covers their anatomy, functions, diseases, and the critical synergy between them — something most medical resources fail to explain as a unified system.
What Is the Liver and What Is the Gallbladder?
Understanding these two organs individually is the first step before exploring how they operate as a team.
The Liver — Your Body's Chemical Factory
- The liver sits in the right upper quadrant of the abdomen, just beneath the diaphragm. It weighs roughly 1.4–1.5 kg in adults, making it the largest solid organ in the human body.
- Anatomically, the liver has two main lobes — the larger right lobe and the smaller left lobe — separated by the falciform ligament. On its visceral (inferior) surface, two additional lobes are visible: the caudate lobe and the quadrate lobe.
- A critical landmark is the porta hepatis, the gateway on the liver's underside where the portal vein, hepatic artery, and common hepatic duct enter and exit.
- The liver has a unique dual blood supply: approximately 75–80% of its blood comes from the portal vein (nutrient-rich blood from the intestines), while the remaining 20–25% arrives via the hepatic artery (oxygen-rich blood). This arrangement makes the liver ideally positioned to process nutrients and filter toxins immediately after absorption from the gut.
At the cellular level, the functional units of the liver are hepatic lobules — hexagonal clusters of hepatocytes arranged around a central vein. Each lobule contains sinusoidal capillaries lined with Kupffer cells (specialized immune cells) and receives bile canaliculi that drain bile toward the bile ducts. The canals of Hering connect these tiny canaliculi to the larger intrahepatic bile duct system.
One truly remarkable feature: the liver can regenerate. Studies show that even after surgical removal of up to 70% of liver tissue, the organ can regrow to its original functional capacity within weeks. No other internal organ possesses this ability to such an extent.
The Gallbladder — A Small Organ With a Big Role
The gallbladder is a hollow, pear-shaped organ approximately 7–10 cm long, sitting in a shallow fossa on the liver's visceral surface. It has a capacity of about 30–50 mL of bile and is anatomically divided into three parts: the fundus (the rounded bottom), the body (the main portion), and the neck (the narrow end that connects to the cystic duct).
The gallbladder wall has distinctive layers — a mucosal lining with extensive folds (rugae) covered in microvilli for absorption, a muscular layer for contraction, and a serosal outer covering. Unlike many parts of the GI tract, the gallbladder lacks a true submucosa. Its blood supply comes primarily from the cystic artery, usually a branch of the right hepatic artery.
Innervation involves both divisions of the autonomic nervous system: sympathetic fibers from the celiac and superior mesenteric plexuses and parasympathetic fibers from the vagus nerve. This dual innervation controls both bile storage during fasting and bile ejection after meals.
Liver and Gallbladder Difference — A Quick Comparison
| Feature | Liver | Gallbladder |
|---|---|---|
| Size | ~1.4–1.5 kg, largest internal organ | 7–10 cm long, ~30–50 mL capacity |
| Location | Right upper abdomen, under diaphragm | Inferior surface of right liver lobe |
| Primary Function | Bile production, detoxification, metabolism | Bile storage and concentration |
| Blood Supply | Portal vein (75–80%) + hepatic artery (20–25%) | Cystic artery |
| Regeneration | Can regenerate up to 70% of lost tissue | Cannot regenerate |
| Can You Live Without It? | No — liver failure is fatal | Yes — bile drains directly into intestine |
| Common Diseases | Hepatitis, cirrhosis, fatty liver, liver cancer | Gallstones, cholecystitis, gallbladder cancer |
How Do the Liver and Gallbladder Function Together?
This is where most resources fall short. They treat the liver and gallbladder as seperate topics. In reality, they function as a single, integrated biliary system.
Bile Production and Storage
Hepatocytes in the liver continuously produce 800–1,000 mL of bile per day. This golden-green fluid contains water, bile salts (synthesized from cholesterol), bilirubin (a breakdown product of hemoglobin), cholesterol, phospholipids (mainly lecithin), and electrolytes.
Between meals, the sphincter of Oddi — a muscular valve at the junction where the common bile duct meets the duodenum — remains closed. This forces bile to back up into the cystic duct and fill the gallbladder. Inside the gallbladder, bile is concentrated by up to 5–10 fold through active absorption of water and electrolytes by the mucosal epithelium.
The Bile Ejection Mechanism
- When fatty food enters the duodenum, enteroendocrine cells (I-cells) release cholecystokinin (CCK).
- This hormone triggers two simultaneous events:
- 1.Gallbladder contraction — smooth muscle in the gallbladder wall contracts, squeezing concentrated bile into the cystic duct
- 2.Sphincter of Oddi relaxation — the valve opens, allowing bile to flow into the duodenum
The vagus nerve (parasympathetic) also contributes to gallbladder contraction during the cephalic phase of digestion — meaning just the sight or smell of food can initiate mild bile release.
Enterohepatic Circulation — The Recycling Loop
Here's something fasinating: your body doesn't waste bile acids. After bile salts help emulsify fats in the duodenum and jejunum, approximately 95% are reabsorbed in the terminal ileum through specialized sodium-dependent transporters. These recycled bile acids travel via the portal vein back to the liver, where hepatocytes re-secrete them into bile. This enterohepatic circulation cycles bile salts 6–8 times per day, allowing the body to maintain an adequate bile acid pool (~3–5 grams) despite producing only about 0.5 grams of new bile acids daily.
The Biliary Tract — Connecting the System
The biliary ductal system is the highway connecting liver, gallbladder, and intestine:
- Right and left hepatic ducts → merge to form the common hepatic duct
- Cystic duct (from the gallbladder) joins the common hepatic duct → forming the common bile duct (CBD)
- The CBD descends behind the duodenum and often merges with the main pancreatic duct at the ampulla of Vater (hepatopancreatic ampulla)
- The sphincter of Oddi controls flow into the duodenum
This shared anatomy between the biliary and pancreatic systems explains why gallstone complications can trigger pancreatitis — a stone impacted at the ampulla of Vater can block both bile and pancreatic juice drainage.
Liver Functions Beyond Bile — Why It's Called the Body's Powerhouse
- While bile production is the liver's most direct link to the gallbladder, the liver performs over 500 different functions.
- Here are the major ones:
Metabolic and Synthetic Functions
- Protein synthesis: the liver produces albumin (maintains blood osmotic pressure), clotting factors (fibrinogen, prothrombin), and complement proteins
- Carbohydrate metabolism: stores glucose as glycogen (~100g stored), performs gluconeogenesis during fasting
- Lipid metabolism: synthesizes cholesterol, lipoproteins (VLDL, HDL), and converts excess carbohydrates to triglycerides
- Vitamin storage: stores fat-soluble vitamins A, D, and K, plus vitamin B12 and iron (as ferritin)
Detoxification and Drug Metabolism
The liver is the primary site of first-pass metabolism — drugs absorbed from the gut pass through the liver via the portal vein before reaching systemic circulation. Cytochrome P450 enzymes in hepatocytes chemically modify these substances, making them water-soluble for excretion. This is why liver disease can dramatically alter drug dosing requirements.
Bile acids themselves influence drug bioavailability — some medications require bile for proper absorption, while others are excreted through bile (enterohepatic cycling of drugs). This is a connection between liver, gallbladder, and pharmacology that few resources mention.
Endocrine and Immune Roles
The liver produces insulin-like growth factor 1 (IGF-1) in response to growth hormone, converts thyroxine (T4) to the more active triiodothyronine (T3), and synthesizes angiotensinogen (part of blood pressure regulation). Kupffer cells in the liver sinusoids act as resident macrophages, filtering bacteria and debris from portal blood — an important immune defense against gut-derived pathogens.
What Are Common Issues That Affect the Liver and Gallbladder?
Gallstones (Cholelithiasis) — Types and Risk Factors
- Gallstones affect approximately 10–15% of adults in Western countries, with prevalence rising in India due to dietary changes.
- There are two main types:
Cholesterol Stones
- Account for about 80% of gallstones.
- They form when bile becomes supersaturated with cholesterol — meaning more cholesterol is present than bile salts and lecithin can keep in solution. Risk factors include obesity, rapid weight loss (losing >1.5 kg/week), female sex, pregnancy, age over 40, and certain medications (estrogen therapy, fibrates).
A 2012 study published in Hepatology confirmed that obesity increases hepatic cholesterol secretion, directly contributing to bile supersaturation and stone formation.
Pigment Stones
These are either black (associated with hemolytic anemias, cirrhosis, and chronic liver disease — formed in the gallbladder) or brown (associated with biliary infections and stasis — often formed in the bile ducts). Black pigment stones are composed primarily of calcium bilirubinate, while brown stones contain bacterial degradation products.
Biliary Sludge — The Precursor
Biliary sludge is a thick mixture of mucus, cholesterol crystals, and calcium bilirubinate granules that accumulates in the gallbladder during prolonged fasting, pregnancy, or parenteral nutrition. It's considered a precursor to gallstone formation and can itself cause biliary pain. Sludge resolves spontaneously in some patients but progresses to stones in roughly 5–15% of cases.
What Are the First Signs of a Bad Gallbladder?
The most common early symptom is biliary colic — episodic pain in the right upper quadrant (RUQ) or epigastric area, often radiating to the right shoulder blade. This pain typically occurs 30–60 minutes after a fatty meal and can last several hours.
Other warning signs include:
- Nausea and vomiting during pain episodes
- Bloating and intolerance of fatty foods
- Indigestion that doesn't respond to antacids
If infection develops, you may notice fever, persistent pain lasting more than 6 hours, and tenderness on pressing the RUQ (positive Murphy's sign). Jaundice (yellowing of skin and eyes) suggests a stone has migrated into the common bile duct.
Cholecystitis — When the Gallbladder Becomes Inflamed
Acute cholecystitis develops when a gallstone obstructs the cystic duct, causing gallbladder distension, inflammation, and sometimes bacterial infection. If untreated, it can progress to gallbladder perforation, abscess, or gangrene. Chronic cholecystitis involves repeated episodes of inflammation that scar and stiffen the gallbladder wall.
Gallstone Ileus — A Rare but Serious Complication
In elderly patients, a large gallstone can erode through the gallbladder wall into the adjacent small intestine (forming a cholecystoenteric fistula) and then travel down to obstruct the narrowest part of the small bowel — usually the ileocecal valve. This is called gallstone ileus and, though uncommon, carries significant mortality if not surgically treated.
Gallbladder Cancer
- Gallbladder cancer is rare globally but notably more common in certain populations, including Northern India. It's often discovered incidentally during cholecystectomy.
- Symptoms — when present — mimic chronic cholecystitis (RUQ pain, weight loss, jaundice), making early detection challanging. Porcelain gallbladder (calcification of the wall) and large polyps (>1 cm) are considered risk factors.



Hepatitis Jaundice Fatty liver disease


स्वयं दवा न लें और प्रतीक्षा न करें। अभी डॉक्टर से चैट शुरू करें
Liver disease Biliary dyskinesia
How to Tell If It's Liver or Gallbladder Pain?
This is one of the most commonly searched questions — and understandably so, since both organs occupy the same anatomical neighborhood.
| Feature | Liver Pain | Gallbladder Pain |
|---|---|---|
| Location | Diffuse RUQ, may extend across upper abdomen | Focused RUQ or epigastric, radiates to right shoulder |
| Character | Dull, aching, persistent | Sharp, colicky, comes in waves |
| Timing | Constant, worsens over weeks | Episodic, often after fatty meals |
| Associated Symptoms | Fatigue, itching, spider angiomas, ascites | Nausea, vomiting, food intolerance |
| Jaundice Pattern | Hepatic (elevated ALT/AST) | Obstructive (elevated ALP, direct bilirubin) |
| Key Diagnostic Test | Liver function tests + ultrasound/FibroScan | Abdominal ultrasound (gold standard for stones) |
Diagnostic Approaches
- Ultrasound: first-line for gallstones (sensitivity >95%) and liver abnormalities
- CT scan: better for complications like perforation, abscess, or tumors
- MRCP (Magnetic Resonance Cholangiopancreatography): non-invasive imaging of the bile ducts
- ERCP (Endoscopic Retrograde Cholangiopancreatography): both diagnostic and therapeutic — can remove stones from the common bile duct
- Endoscopic ultrasound (EUS): detects small stones and sludge missed by standard ultrasound
- FibroScan: assesses liver fibrosis non-invasively
Are Gallbladder and Liver Problems Related? The Synergy Nobody Explains
- This is perhaps the biggest gap in existing medical content online.
- The liver and gallbladder don't just share plumbing — diseases of one organ directly cause or worsen diseases of the other.
How Liver Disease Affects the Gallbladder
- Cirrhosis increases the prevalence of pigment gallstones by 2–5 times. Portal hypertension alters bile composition and gallbladder motility, creating conditions ripe for stone formation
- Non-alcoholic fatty liver disease (NAFLD) changes bile acid metabolism, increasing cholesterol saturation of bile. A 2012 study in BMC Gastroenterology found that gallstone disease was associated with more severe liver damage in patients with NAFLD
- Hepatitis (viral or alcoholic) disrupts bilirubin metabolism, potentially increasing unconjugated bilirubin in bile and promoting pigment stone formation
How Gallbladder Disease Affects the Liver
- Choledocholithiasis (stones in the common bile duct) causes obstructive jaundice — backed-up bile damages hepatocytes and, if prolonged, leads to secondary biliary cirrhosis
- Ascending cholangitis occurs when bacteria travel up the obstructed bile duct, causing life-threatening infection. It can lead to hepatic abscesses
- Mirizzi syndrome: a gallstone impacted in the cystic duct or gallbladder neck compresses the common hepatic duct externally, mimicking a bile duct tumor
Understanding Jaundice Through This Lens
Jaundice — the yellowing of skin and sclerae due to elevated bilirubin — can be classified by origin:
- Pre-hepatic: excess bilirubin production (hemolysis) — unconjugated hyperbilirubinemia
- Hepatic: liver dysfunction (hepatitis, cirrhosis) — mixed hyperbilirubinemia
- Post-hepatic (obstructive): bile duct blockage (gallstones, tumors) — conjugated hyperbilirubinemia with pale stools and dark urine
Differentiating these types is essential because treatment differs dramatically — medical therapy for hepatic causes versus surgical or endoscopic intervention for obstructive causes.
Treatment — Cholecystectomy and Life Without a Gallbladder
Surgical Options
Laparoscopic cholecystectomy is the gold standard treatment for symptomatic gallstones — performed through 3–4 small incisions, with most patients going home the same day. Recovery typically takes 1–2 weeks. Open cholecystectomy is reserved for complicated cases (severe inflammation, unclear anatomy, suspected cancer). Robotic-assisted cholecystectomy is gaining traction in some centers, offering enhanced dexterity and visualization.
For patients unfit for surgery, ERCP with sphincterotomy can remove common bile duct stones, and oral dissolution therapy with ursodeoxycholic acid (UDCA) may slowly dissolve small cholesterol stones over 6–24 months — though recurrence rates are high.
Can You Live Without a Gallbladder?
- Absolutely. After cholecystectomy, bile flows directly from the liver into the duodenum through the common bile duct. However, without the gallbladder's concentrating function, bile is delivered in a more dilute, continuous stream rather than in concentrated bursts.
- This can cause:
- Postcholecystectomy diarrhea in about 10–15% of patients (due to excess bile acids reaching the colon)
- Temporary fat malabsorption and bloating
Diet After Cholecystectomy
- Limit dietary fat to approximately 30% of total calories for the first 4–6 weeks
- Introduce high-fiber foods gradually to avoid bloating
- Eat smaller, more frequent meals rather than large ones
- Most patients return to a completely normal diet within 2–3 months

What Foods Trigger Gallbladder Issues?
- Diet plays a significant role in both preventing and managing gallbladder problems.
- Foods and habits that increase risk include:
- High-fat foods: fried foods, full-fat dairy, fatty cuts of meat, butter, and cream-based sauces trigger strong CCK release and gallbladder contraction — painful if stones are present
- Refined carbohydrates: white bread, pastries, and sugary drinks increase hepatic cholesterol secretion
- Rapid weight loss: crash diets or bariatric surgery can mobilize large amounts of cholesterol into bile. Losing more than 1.5 kg per week significantly increases gallstone risk
- Prolonged fasting: gallbladder stasis promotes sludge and stone formation
Protective factors include regular physical activity, gradual weight management, adequate fiber intake, moderate coffee consumption (studies suggest 2–3 cups daily may reduce gallstone risk by up to 25%), and healthy fats like olive oil and omega-3 fatty acids.
Liver and Gallbladder Supplements — Do They Help?
- Many people search for supplements to "cleanse" or support the liver and gallbladder.
- Here is what evidence actually supports:
- Milk thistle (silymarin): the most studied liver supplement. A 2017 meta-analysis in Phytotherapy Research showed modest reductions in liver enzymes (ALT, AST) in patients with NAFLD, but evidence remains limited for other liver conditions
- Artichoke leaf extract: may stimulate bile flow (choleretic effect) and has shown some benefit for dyspeptic symptoms in clinical trials
- Ursodeoxycholic acid (UDCA): technically a medication, not a supplement — used to dissolve small cholesterol gallstones and treat primary biliary cholangitis
- Turmeric (curcumin): anti-inflammatory properties may benefit liver health, but bioavailability is poor without piperine. Some evidence suggests curcumin stimulates gallbladder contraction
- "Liver cleanses" and "gallbladder flushes": typically involving olive oil and lemon juice — no credible evidence supports these. The "stones" passed are usually saponified oil, not actual gallstones
> Important: Always consult a qualified healthcare provider before starting any supplement, especially if you have existing liver or gallbladder disease.
FAQ — Liver and Gallbladder
Where is the liver and gallbladder located in the body?
Both are in the right upper quadrant of the abdomen. The liver sits directly beneath the diaphragm, spanning across the midline slightly into the left upper quadrant. The gallbladder is nestled on the undersurface of the liver's right lobe, in a small depression called the gallbladder fossa.
How does the gallbladder help other organs?
- The gallbladder supports the small intestine by delivering concentrated bile for fat emulsification and absorption of fat-soluble vitamins (A, D, E, K).
- It indirectly supports the pancreas — bile and pancreatic juice enter the duodenum at the same location (ampulla of Vater), and proper bile flow helps prevent pancreatic duct obstruction.
What does liver and gallbladder pain look like in a picture?
Pain from both organs is felt in the right upper quadrant, but gallbladder pain classically radiates to the right shoulder or between the shoulder blades (referred pain via the phrenic nerve). Liver pain tends to be more diffuse and may be accompanied by abdominal distension if ascites is present.
Can liver problems cause gallstones?
Yes. Cirrhosis increases gallstone prevalence by 2–5 times. Fatty liver disease alters bile composition, and chronic liver disease can impair gallbladder motility — all of which promote stone formation.
What is the role of the liver and gallbladder in drug metabolism?
The liver performs first-pass metabolism of orally ingested drugs using cytochrome P450 enzymes. Some metabolized drugs are excreted into bile and may undergo enterohepatic recirculation — being reabsorbed in the intestine and returning to the liver. The gallbladder's role in concentrating bile can affect the timing and intensity of biliary drug excretion.
Can the liver regenerate after damage?
Yes. The liver is the only internal organ capable of substantial regeneration. After partial hepatectomy (removal of up to 70%), the remaining liver tissue undergoes compensatory hyperplasia, typically restoring full functional capacity within 8–15 days in animal models and several weeks in humans.

Final Thoughts — Protect Both Organs Together
The liver and gallbladder are not two seperate stories — they are chapters in the same book. What harms one almost inevitably impacts the other, and understanding this connection is essential for prevention, early diagnosis, and effective treatment.
Practical steps to protect both organs: maintain a healthy weight without crash dieting, eat a balanced diet rich in fiber and healthy fats, stay physically active, limit alcohol consumption, avoid unnecessary medications, and don't ignore persistent upper abdominal pain. Early diagnosis through simple blood tests (liver function panel) and abdominal ultrasound can catch problems before they become emergencies.
If you're experiencing symptoms like right upper quadrant pain, unexplained fatigue, jaundice, or changes in stool color — don't wait. Consult a qualified healthcare provider who can evaluate both your liver and gallbladder as the interconnected system they truly are.
Scientific Sources
- Ginsenoside Rg1 alleviates ANIT-induced cholestatic liver injury by inhibiting hepatic inflammation and oxidative stress via SIRT1 activation — Gao Q et al., 2024, Journal of ethnopharmacology
- Cholesterol and Immune Microenvironment: Path Towards Tumorigenesis — Saad EE et al., 2024, Current nutrition reports
- Promising traditional Chinese medicine for the treatment of cholestatic liver disease process (cholestasis, hepatitis, liver fibrosis, liver cirrhosis) — Wei C et al., 2022, Journal of ethnopharmacology
- Liver and gall bladder channel parallels in the Hippocratic Corpus and Huang Di Nei Jing with theoretical considerations — Paulo RF et al., 2022, Journal of traditional and complementary medicine
- The Genus Rumex: Review of traditional uses, phytochemistry and pharmacology — Vasas A et al., 2015, Journal of ethnopharmacology
- Study on preparation technology of Qi Yu constitution Yangsheng granules — Zhong F et al., 2024, Technology and health care : official journal of the European Society for Engineering and Medicine
- Integrated metabolomics and network pharmacology to explore the mechanism of Huzhang Erjin Decoction against ANIT-induced cholestatic hepatitis — Li S et al., 2025, Journal of ethnopharmacology
- Investigating therapeutic effects and the underlying mechanisms of jia-wei-yin-chen-hao-tang in non-alcoholic fatty liver disease based on network pharmacology analysis and experimental validation — Zhou RY et al., 2025, Journal of ethnopharmacology
- Pomegranate seeds: a comprehensive review of traditional uses, chemical composition, and pharmacological properties — Wang J et al., 2024, Frontiers in pharmacology
- Research Progress of Eucommia ulmoides Oliv and Predictive Analysis of Quality Markers Based on Network Pharmacology — Zhao X et al., 2024, Current pharmaceutical biotechnology
- Helichrysum italicum: from traditional use to scientific data — Antunes Viegas D et al., 2014, Journal of ethnopharmacology
- Curcumae Radix: a review of its botany, traditional uses, phytochemistry, pharmacology and toxicology — Ao M et al., 2022, The Journal of pharmacy and pharmacology
- The therapeutic potential of milk thistle in diabetes — Kazazis CE et al., 2014, The review of diabetic studies : RDS
- Quality Markers' Discovery and Quality Evaluation of Jigucao Capsule Using UPLC-MS/MS Method — He Y et al., 2023, Molecules (Basel, Switzerland)
- Pharmacological Activities and Synthesis of Esculetin and Its Derivatives: A Mini-Review — Liang C et al., 2017, Molecules (Basel, Switzerland)
- Prunella vulgaris L. attenuates gut dysbiosis and endotoxin leakage against alcoholic liver disease — Rao PL et al., 2024, Journal of ethnopharmacology
- Swertia L.: A comprehensive review of its genetic relationship, chemical compositions, pharmacological effects, toxicities, and applications — Guo S et al., 2023, Phytotherapy research : PTR
- Prunella vulgaris L. - A Review of its Ethnopharmacology, Phytochemistry, Quality Control and Pharmacological Effects — Pan J et al., 2022, Frontiers in pharmacology
- [[Scientific connotation of Zangfu theory in traditional Chinese medicine from modern biological research on "organ crosstalk"]](https://pubmed.ncbi.nlm.nih.gov/39701695/) — Wang WY et al., 2024, Zhongguo Zhong yao za zhi = Zhongguo zhongyao zazhi = China journal of Chinese materia medica
- MrgX2-targeted ligand screening from Artemisia capillaris Thunb. extract and receptor-ligand interaction analysis based on MrgX2-HALO-tag/CMC — Jiang Y et al., 2024, Journal of chromatography. B, Analytical technologies in the biomedical and life sciences
उपयोगकर्ताओं के प्रश्न
Can liver disease make gallstones more likely to develop?
Summer
7 दिनों पहले
Yep, liver disease can increase the risk of developing gallstones. Conditions like cirrhosis raise the chances of pigment stones forming. It seems that liver problems may also influence bile composition and flow, which could contribute to gallstone formation. So yeah, keeping the liver healthy is definitely a piece of the puzzle!
What are gallstones and how do they form in the liver?
Vada
16 दिनों पहले
Gallstones are hard deposits that form in the gallbladder, not the liver. They're mainly cholesterol stones, happening when bile gets too rich with cholesterol. Think of it like the bile can't keep the cholesterol mixed in, so it crystallizes. Lifestyle and diet changes in places like India are upping the risk!
What are the common symptoms of chronic cholecystitis that I should be aware of?
Vada
24 दिनों पहले
Chronic cholecystitis can be sneaky, but common symptoms to look out for include that nagging RUQ (right upper quadrant) pain, feeling bloated, nausea, vomiting, and sometimes even weight loss. It can also lead to jaundice if bile flow is blocked. But be careful—symptoms can overlap with other conditions, so always good to consult a healthcare professional for a proper check-up!
How does stress management in Ayurveda specifically benefit liver health?
Jack
39 दिनों पहले
Managing stress is super important in Ayurveda for better liver health! When we're stressed, the body produces toxins that can strain the liver. Stress management techniques like meditation, yoga, and pranayama help balance your doshas and improve agni, or digestive fire, which in turn helps the liver process and detoxifies more effectively. It's all about holistically keeping your inner harmony!
Can I detox my liver with Ayurveda if I have a busy lifestyle?
Evelyn
49 दिनों पहले
Absolutely, you can detox your liver with Ayurveda even with a busy lifestyle! Simple steps like daily warm lemon water, including herbs like turmeric in your diet, and staying hydrated can make a big difference. Try short meditation or breathing exercises for stress, and aim for moderate exercise. It's all about small, consistent habits. 😊
Is it safe to consume alcohol in moderation if I'm following an Ayurvedic liver health program?
Caleb
58 दिनों पहले
Even in moderation, alcohol can be tricky when you're on an Ayurvedic liver health program. Alcohol might aggravate pitta and affect agni (digestive fire), which we want to keep balanced. It’s best to stick to non-alcoholic drinks, maybe herbal teas or infused water. But hey, everyone's different—observing how your body responds is key!
How can regular hydration impact liver function according to Ayurvedic principles?
Bella
68 दिनों पहले
Proper hydration in Ayurveda helps maintain balance in the body's doshas and support agni (digestive fire), which is crucial for liver health. When you're well-hydrated, it can aid in detoxification and ensure smooth functioning of liver. Think of it like keeping oil in an engine—everything runs smoothly! Just make sure you sip water through the day, not chug it all at once.
Is it safe to combine regular exercise with Ayurvedic practices for liver health?
Presley
78 दिनों पहले
Totally safe to combine regular exercise with Ayurvedic practices for liver health! Exercise boosts circulation, detoxifies the body, and supports the liver. Just make sure to match it to your dosha type. Vata types can do calming exercise like yoga, while Kapha might enjoy more vigorous activities. Keep it balanced with good hydration and rest!
Can I use Panchakarma for liver detoxification at home or should I go to a professional?
Luke
87 दिनों पहले
Doing Panchakarma at home can be tricky and not really recommended. It's a deep detox process that needs professional guidance to be safe and effective. The therapies are complex, and its best to have expert assess your unique health and dosha needs. So, seek help from a trained Ayurvedic practicioner!
Are there any specific Ayurvedic practices for detoxifying the liver after heavy alcohol consumption?
Avery
170 दिनों पहले
Yes, for detoxifying the liver after heavy alcohol use, Ayurveda suggests focusing on herbs like neem and guduchi, which can support liver health. Drinking plenty of warm water and incorporating turmeric into your diet might help, too. Some gentle yoga could improve blood flow and help the liver cleanse itself. It's good to aim for balance and improve digestion with light meals like khichdi. Always check with a practitioner for personalized advice!
संबंधित आलेख

Gastrointestinal Disorders
Arshoghni Vati Uses – Ayurvedic Remedy for Piles and Hemorrhoids
Discover the benefits and uses of Arshoghni Vati, a powerful Ayurvedic remedy for piles (hemorrhoids). Learn how it helps alleviate symptoms and promotes rectal health.
3,446

Gastrointestinal Disorders
What Causes Constipation: Ayurvedic Reasons, Symptoms, and Treatment
What causes constipation? Learn Ayurvedic causes, symptoms, danger signs, and natural remedies for chronic and severe constipation, including diet and lifestyle tips
2,024

Gastrointestinal Disorders
Vilwadi Lehyam Uses, Dose, Side Effects and Ingredients
Exploration of Vilwadi Lehyam Uses, Dose, Side Effects and Ingredients
2,413

Gastrointestinal Disorders
Is Banana Good for Loose Motion, Diarrhea, or Indigestion?
Learn if banana is good for loose motion, diarrhea, or indigestion. Discover how bananas help in stopping loose motion and soothe digestive issues naturally
6,408

Gastrointestinal Disorders
कामधेनु रस
कामधेनु रस की खोज
1,908

Gastrointestinal Disorders
IBS Treatment in Ayurveda: What Actually Helps When Your Gut’s a Mess
Let’s be honest. If you’re googling "IBS treatment in Ayurveda," you’re probably desperate. Because Irritable Bowel Syndrome is one of those things that makes you feel like your body is sabotaging you from the inside out. And all the antispasmodics and lo
2,855

Gastrointestinal Disorders
लिवोकॉट टैबलेट के उपयोग, खुराक, सामग्री, साइड इफेक्ट्स
लिवोकॉट टैबलेट के उपयोग, खुराक, सामग्री, और साइड इफेक्ट्स की जानकारी
2,049

Gastrointestinal Disorders
Best Ayurvedic Medicine for Weight Gain: Comprehensive Guide
Discover the best Ayurvedic medicine for weight gain, backed by research and expert insights. Learn how natural remedies can support healthy, sustainable gains.
5,110

Gastrointestinal Disorders
महाशंख वटी के फायदे, खुराक, सामग्री, साइड इफेक्ट्स
महाशंख वटी के फायदे, खुराक, सामग्री, और साइड इफेक्ट्स की जानकारी
7,841

Gastrointestinal Disorders
Ayurvedic Medicine for Blood Clots: A Science-Based Overview
Explore how ayurvedic medicine for blood clot prevention complements modern therapies. Learn about research, best practices, and safe usage.
3,910
विषय पर संबंधित प्रश्न
क्या मैं वजन बढ़ाने की कोशिश करते समय एसिड रिफ्लक्स के लिए फुल फैट दूध का इस्तेमाल कर सकता हूँ?
11 दिनों पहले
एक बुजुर्ग मरीज में, जिसे डुओडेनल अल्सर का इतिहास है, पुरानी एसिडिटी और कमजोरी का इलाज कैसे करें?
11 दिनों पहले
किण्वन कोलाइटिस और शुरुआती विटिलिगो का इलाज आयुर्वेदिक उपायों से कैसे करें?
11 दिनों पहले
अतिरिक्त दस्तावेज़
© 2024 Ask Ayurveda. सर्वाधिकार सुरक्षित।